The hypopharynx is the lower or most inferior portion of the pharynx, and it communicates the oropharynx with the esophageal inlet. The larynx indents the anterior wall of the hypopharynx to form a horseshoe-shaped hollow cavity. This creates a central communal aerodigestive passageway and two lateral fossae (i.e., the pyriform sinuses). The hypopharyngeal walls are composed of four layers of tissue: mucosa, fibrous fascia, muscular layer, and areolar coat. The entire wall thickness is less than 1 cm and generally provides little, if any, hindrance to tumor penetration.
The mucous membrane has an epithelial surface exposed to air (respiratory function), which is lined by ciliated pseudostratified columnar epithelium; the surfaces that allow the transport of both food and air or food only are lined with stratified squamous epithelium. These differences have importance in the type and differentiation of malignancies occurring in various parts of the pharynx. The muscular layer of the hypopharynx is composed of two paired constrictor muscles, the middle and inferior constrictors. These muscles attach anteriorly to the hyoid bone and thyroid cartilage and fuse posteriorly with each other. The inferior constrictor muscle overlaps the middle constrictor muscle. The inferior constrictor muscle has two specialized divisions; the first is the cricopharyngeus muscle, which is composed of the lowermost fibers and is the sphincteric guardian of the esophagus. The inferior border of the cricopharyngeus muscle is the inferior border of the hypopharynx. The second specialized muscle forms the cricothyroid muscle, which is the tensor of the vocal folds. This muscle lies on the cricoid lamina and inserts into the thyroid cartilage (Fig. 41-1).

The cricothyroid muscle is innervated by the external branch of the superior laryngeal nerve. The outer coat of the hypopharynx is the areolar tissue, which fuses with the deep cervical fascia or the buccopharyngeal fascia. Between this areolar fascia and the prevertebral fascia, which covers the longitudinal spinous muscles (longus colli and longus capitis), is a potential space (retropharyngeal space) that may act as a conduit for tumor extension.
The areolar layer contains the vessels, nerves, and lymphatics that travel lateral to the pharyngeal walls in a potential parapharyngeal space of loose connective tissue surrounded by the deep cervical and visceral fascia.
The arterial supply of the hypopharynx is mainly from the paired ascending pharyngeal arteries, superior thyroid arteries, and branches from the lingual artery, all divisions of the external carotid system. A venous plexus drains the pharynx (including the palate and tonsil) and communicates with the internal jugular vein.
The lymphatics of the hypopharynx generally travel in a cephalad direction, through the thyrohyoid membrane toward the upper deep cervical lymph nodes, to enter the jugulodigastric lymph nodes and the upper and middle jugular chain. There is also free communication with the spinal accessory lymph nodes and retropharyngeal nodes; in this group the highest nodes (Rouviere) are at the skull base. This close proximity of the lymphatics to the mucosa partly explains the high incidence of early metastases. The lowest portions of the hypopharynx (the postcricoid region, pyriform apex, and inferior hypopharynx) drain into a lymphatic chain that follows the recurrent laryngeal nerve to the paratracheal, paraesophageal, and supraclavicular nodes.
The motor neural supply of the hypopharyngeal muscles is from the pharyngeal plexus of nerves, which are motor-neural fibers from the glossopharyngeal (IX) and vagus (X) nerves. The inferior hypopharynx is innervated by branches from the recurrent laryngeal nerve (X). Efferent pain fibers traveling with the internal branch of the superior laryngeal nerve through the auricular branch of the vagus (nerve of Arnold) to the ipsilateral ear cause pain, usually an ill-defined, dull ache in the superior-posterior wall of the external auditory canal or the posterior skin of the pinna.
Clinically the hypopharynx is separated from the rest of the pharynx by various anatomic landmarks. The superior border arises anteriorly at the base of the vallecula (inferior border of the hyoid bone) and proceeds laterally to the pharyngoepiglottic folds (epithelial covering of the pharyngoepiglottic muscle). The superior border posteriorly is an imaginary plane connecting these points with the
posterolateral pharyngeal wall at the level of the fourth cervical vertebra. The posterior and lateral hypopharyngeal walls are continuous with those of the oropharynx without distinct anatomic separation. The medial wall is formed by the lateral border of the epiglottis, the aryepiglottic folds (epithelial covering of the aryepiglottic muscles and free edge of the quadrangular ligament), and
lateral laryngeal wall (mucosa-covered cricothyroid muscle). The anterior border is the postcricoid region, which extends from the interarytenoid area (mucosa-covered interarytenoid transverse and oblique muscles) and cricothyroid muscle. The inferior border is at the inferior edge of the pharyngeal aponeurosis and its cricopharyngeal ligament. The latter is at the inferior border of the cricopharyngeal muscle and the superior edge of the longitudinal and circular esophageal muscles (i.e., the esophageal inlet) (Fig. 41-1).
The hypopharynx is further subdivided clinically into three partitions: the pyriform fossae, the posterolateral pharynx, and the postcricoid region (Fig. 41-2).

The posterior border of the larynx forms the postcricoid region. The area extends from the level of the arytenoids to the inferior edge of the cricoid cartilage. The posterolateral pharynx extends from the level of the hyoid bone to the inferior border of the cricopharyngeus muscle. The pyriform fossa lies lateral to the larynx. The medial wall is formed by the aryepiglottic fold and the lateral laryngeal wall (cricothyroid muscle). The anterior and lateral walls are formed by the thyroid ala. The posterior wall is open and communicates fully with the hypopharyngeal lumen. The pyriform fossa apex lies below the level of the vocal cords and occasionally below the cricoid cartilage. Thus, tumors that extend to the pyriform fossa apex or postcricoid area are not amenable to conservation voice-sparing surgical procedures.
Epidemiology
The number of new pharyngeal carcinomas in the United States is slowly rising. In 1997, approximately 8890 new cases were reported (6400 in men and 2400 in women). [ref: 81] At the time of clinical presentation, approximately 37% of patients have local disease, 43% regional disease, and 10% distant metastases.
Both tobacco and alcohol are important cofactors for hypopharyngeal carcinomas. [ref: 9] In Southwestern Asia, the habit of chewing betel quid and areca nuts is an important cofactor for hypopharyngeal cancers. The risk is 35-fold greater for those who smoke two or more packs of cigarettes per day and drink more than 4 ounces of alcohol per day; 89% of patients with pyriform fossa cancers and 83% of those with aryepiglottic fold cancers have a previous history of smoking and alcohol use. The incidence of second primary tumors, with more than 20 years of follow-up, was 6.2% and 8%, respectively. [ref: 97,99] This is a much lower incidence than reported by Schwartz and associates. [ref: 90] They reported a similar high usage of cigarettes and alcohol, with a 19% incidence of second primary tumors. Generally, black tobaccos have higher tumorgenicity than blond tobaccos. [ref: 79,103]
The mean age for patients with hypopharyngeal tumors ranges from 60 to 65 years. In our patients, age distributions were as follows: pyriform fossa tumors, 29 to 83 years (mean 60.3 years; median 59 years), aryepiglottic fold tumors, 39 to 87 years (mean 62.4 years; median years), and pharyngeal wall tumors, 37 to 85 years (mean 63 years; median 63 years).
Although in the past the overall incidence of hypopharyngeal carcinomas was greater in men than in women by a ratio of 7:1, today this differential is declining to a male:female ratio of 5:1. [ref: 97,99] In the United States, the ratio of men to women is 3:1 to 4:1 for pharyngeal wall and 3:1 for postcricoid tumors. Postcricoid tumors are relatively rare in the United States. Although cancers of the
upper hypopharynx are associated with smoking and alcohol consumption, those of the lower hypopharynx are associated with nutritional deficiencies of iron and possibly vitamin C. In 70% of patients with postcricoid carcinomas there was an associated triad of dysphagia, hypochromic microcytic anemia (iron deficiency), and atrophic gastric mucosa (leading to vitamin B(12) deficiency), known as the Plummer-Vinson syndrome.
Second primary tumors of the aerodigestive tract occur in approximately 26% of patients with hypopharyngeal cancers, indicating the multicentric nature of the tobacco- and alcohol-induced neoplasia of the aerodigastric epithelium exposed to common carcinogens. [ref: 50,105] With pyriform fossa tumors, the 45% incidence of second primary tumors was related to the quantity of tobacco and alcohol consumption. [ref: 90]
Natural History
In the United States, the prevalence of cancers at various sites in the hypopharynx occurs in the following decreasing frequency: pyriform fossa, aryepiglottic fold, pharyngeal walls, and postcricoid region. [ref: 55] Because the hypopharynx is not a particularly sensitive area, tumors reach large size with extensive submucosal spread or cervical lymphatic metastases before definitive signs and symptoms lead to a proper diagnosis (Fig. 41-3).

The high incidence of metastases at presentation does not correspond to the T stage of the tumor except with extensive larger lesions (Table 41-1). In addition, tumors of the hypopharynx that recur usually do so at the primary site and cervical lymphatics within 1 year of surgical treatment. [ref: 64,66] In our patients with aryepiglottic and pyriform fossa tumors, 8% of the locoregional recurrences occurred 6 to 20 years after primary therapy. [ref: 97,99] In addition, 18% of patients developed distant metastases during the follow-up period (31 years). [ref: 97,99] Distant metastases generally appear later than locoregional recurrences; thus, patients may die of locoregional disease before distant metastatic enlargement to a discernible size. Therefore, the incidence of distant metastases is higher in patients whose locoregional disease is controlled than in those with locoregional failures. [ref: 64,66]
Tumor location also influences cure rates. The decremental frequency for survival with hypopharyngeal carcinomas at different sites is aryepiglottic folds, pyriform fossa, pharyngeal walls, and postcricoid region. [ref: 40] Despite most patients presenting with large tumors (82% are T3 or T4 pyriform sinus cancers), T stage influences survival. For example, in pyriform fossa tumors (T1 and T2 exceed T3 and T4 by 28%), there is a significant drop-off in cure rates for T3 and T4 stage disease. The presence of neck metastases influences survival. In pyriform fossa and aryepiglottic fold tumors, the presence of metastases reduces the cure rate by 28% and 26%, respectively (i.e., N0 greater than N+ by 26% to 28%). The size or number of metastases influences survival (higher for N1 than N2 and N3) by an additional 12% to 18%. [ref: 97,99] In addition, the presence of extracapsular tumor spread in the cervical lymph nodes and soft tissues of the necks is of paramount importance in survival. [ref: 10,86]
Patterns of Spread Most hypopharyngeal squamous cell carcinomas at presentation (greater than 80%) are stage III or IV disease and have extensive mucosal or submucosal spread. [ref: 97,99] Tumor spreads with little difficulty beyond the visible clinical presentation.
The incidence of squamous cell carcinomas at various sites in the hypopharynx varies. In the United States, tumors occur in the following decremental frequency: pyriform fossa (more than 65%), postcricoid (20%), and hypopharyngeal wall (10% to 15%). [ref: 16,39,46] Our series of patients, compiled from 1964 to 1991, is similar to that reported in the literature. [ref: 26,97,99] There were 426 pyriform fossa tumors (68%); these comprised the most common hypopharyngeal site involved. Isolated aryepiglottic lesions were rare (57 cases [9%]), but lesions involving the aryepiglottic fold with either supraglottic or medial pyriform wall involvement were more common (329 cases). Hypopharyngeal posterolateral wall tumors were the second most frequent (130 cases [21%]). Postcricoid tumors were least common in our series (39 cases [6%]).
Pyriform Fossa Pyriform fossa tumors have early submucosal spread (on whole-organ histologic sections) beyond the visible boundaries of the presenting lesion and early metastases. [ref: 39,55] We have been able to subdivide these tumors (n = 426) into three groups. The most favourable and least common are single-wall tumors (48 cases [11%]); the least favorable and most extensive tumors involved three walls of the pyriform sinus and pyriform apex and have postcricoid or esophageal extensions (93 cases [22%]). The most common lesions with an intermediate therapeutic response rate involve the medial wall of the pyriform fossa and may invade the aryepiglottic fold, supraglottis, larynx, or pyriform fossa apex (267 cases [63%]). The remaining 4% of patients had distant metastases at presentation. [ref: 97,99]
Medial wall tumors, the most common group, may spread along the mucosal surface to involve the aryepiglottic folds (most common pattern). Sometimes they invade medially and deeply into the false vocal folds and larynx via the paraglottic space (Fig. 41-4) [ref: 70];

involvement of the paraglottic space allows a lesion to behave as a transglottic carcinoma. Free access inferiorly along the medial surface of the thyroid cartilage permits the tumor to exit the larynx through the cricothyroid membrane. [ref: 53,54] Medial extension into the larynx also may cause vocal cord paralysis by direct cricoarytenoid muscle or vocalis muscle invasion or cricoarytenoid joint fixation. Paralysis due to invasion of the recurrent laryngeal nerve is rare. In one histologic serial section study, three of 19 patients had cricoarytenoid joint invasion, and four of 19 had perineural extension of the recurrent laryngeal nerve. [ref: 110]
Cancers of the lateral wall and apex of the pyriform fossa commonly invade the thyroid cartilage and less frequently the cricoid cartilage (Fig. 41-5). [ref: 54,80,110]

The thyroid gland may be involved by tumor spread directly through the thyroid cartilage or cricothyroid membrane or posteriorly around the thyroid ala without thyroid destruction. High-resolution computed tomography (CT) studies are useful in these cases. Among 40 cases with lateral wall involvement (studied by serial section), 20 invaded the thyroid cartilage, and two invaded the cricoid rostrum. [ref: 54]
Pharyngeal Walls The lateral hypopharyngeal walls are continuous with the lateral oropharyngeal walls. Very few early lesions are confined to this site at diagnosis; submucosal spread is noted by edema and infiltration beyond the tumor necrotic center. Tumors tend to spread in a cephalad-caudad direction while they simultaneously deeply penetrate through the constrictor muscles and thyrohyoid membrane to gain access to the neurovascular lateral compartment of the soft tissues of the neck. This direct extension may produce a neck mass below the hyoid bone that can be confused with a metastatic lymph node. Tumors, once they penetrate the constrictor muscle, can spread along the muscle and fascial planes to the base of the skull (the origin and suspension of the constrictor muscles) and along the neurovascular planes following the vagus, glossopharyngeal, and sympathetic nerves. Direct thyroid
gland invasion is common. Superior involvement of the pharyngoepiglottic folds, vallecula, and base of the tongue are common.
Posterior hypopharyngeal wall tumors also spread deeply in a cephalo-caudad direction, but have a tendency to remain on the posterior wall; spread laterally to the hypopharyngeal walls occurs late in the disease to form a circumpharyngeal tumor with constrictor muscle invasion and dysphagia. Direct extension of the prevertebral space can occur, but the cervical vertebrae and skull base (bone) are
usually not invaded. These lesions are associated in 12% to 20% of cases with secondary primary tumors [ref: 16,61] and early metastases to the midjugular and retropharyngeal lymph nodes. [ref: 3,61]
Postcricoid Area Postcricoid carcinomas may be primary or extensions of pyriform apex tumors. Most lesions in our patients were extensions from pyriform apex tumors [ref: 99]; many present with circumferential involvement of the postcricoid and hypopharyngeal walls. These lesions commonly invade the cricoid cartilage, interarytenoid space, and posterior cricohyoid muscle to produce hoarseness. [ref: 110] Because of the tendency for early esophageal spread, some have suggested that these epiesophageal tumors are not hypopharyngeal in origin. [ref: 60] They frequently metastasize to the paratracheal nodes and inferior deep cervical nodes. Involvement of the recurrent laryngeal nerves and cricoarytenoid joint and vocal cord fixation are not uncommon. The incidence of skip lesions or multiple primary tumors is high. Therapeutic failure is usually due to persistence of disease at the cervicoesophageal stump, paratracheal nodes, or esophagotracheal party wall invasion. [ref: 94]
Lymphatic Spread The abundant lymphatics of the hypopharynx, coupled with extensive primary disease at presentation, account for the high incidence of metastases to the regional lymph nodes. [ref: 23,24,30,65,71,89,97,99,105,108] The midcervical lymph nodes are most commonly involved, and the incidence of metastases varies according to the site and origin in the hypopharynx (Table 41-1 and Fig. 41-6). [ref: 61]

The ipsilateral jugulodigastric nodes are usually the first area of metastatic manifestation. [ref: 22] The contralateral submaxillary nodes are the most common contralateral neck site. [ref: 11] Secondary lymphatic chain routes of metastases are to the ipsilateral spinal accessory nodes. The incidence of palpable nodes is greater for pyriform fossa tumors than for postcricoid and hypopharyngeal wall tumors. The incidence of metastases progressively increases with increasing tumor size; however, this association should not be relied on. Occult disease occurs irrespective of T stage in pyriform fossa tumors, with an incidence of 60% for T1 and T2 and 84% for T3 and T4 disease. [ref: 7,11,61]
At the time of diagnosis, 60% to 75% of patients have clinically positive metastatic nodes [ref: 71,85]; approximately 10% to 15% demonstrate bilateral metastases, and 2% to 4% have distant metastases. [ref: 97,99] Delayed metastases to the contralateral neck after surgical treatment alone with a positive ipsilateral neck is 90%. [ref: 7] With posterior pharyngeal wall involvement, the incidence of bilateral metastases may be as high as 60%. [ref: 24] Retropharyngeal node involvement may be as high as 50%. [ref: 41]
In our patients, the incidence of metastases (clinical and subclinical) was 60% with pyriform fossa tumors [ref: 99] and 56.3% with aryepiglottic carcinoma. [ref: 97] In both cases the incidence of distant metastases at presentation was 2% to 4%. [ref: 97,99] The incidence of neck metastases with pharyngeal wall tumors was 73%. [ref: 26] In 3419 patients, the most common metastatic site was in level II (69%), and survival decreased as the level of metastases went from level II (39% survival) to the supraclavicular region (level IV, 21% survival). [ref: 14,56] We noted that pathologically confirmed node metastases decreased survival by 26% to 28% (N0 versus N+) and that the size of nodal disease decreased survival by an additional 12% to 18% (N1 versus N2 and N3). [ref: 97,99] There is a decremental survival rate with progressive nodal disease (N0, 57%; N1, 28%; N2, 6%, N3, 0%) and a higher neck recurrence rate with progressively larger neck metastases (N0, 20%; N1, 37%; N2, 48%; N3, 83%). [ref: 43] The incidence of posterior cervical triangle metastases (level V disease) was 7% with hypopharyngeal cancers, and in 37 of 40 patients (90%) these posterior metastases were in anterior N+ neck disease. [ref: 20] The incidence of paratracheal lymph node metastases was 6.3% with hypopharyngeal tumors and was 71.4% with cervical esophageal involvement. [ref: 111] There is early and extensive extracapsular tumor spread (25% in N0 and 70% in N3 disease) in hypopharyngeal tumors. [ref: 47]
Clinical Presentation
Early hypopharyngeal tumors generally produce a mild, nonspecific sore throat or vague discomfort on swallowing, which persists for longer than 2 weeks. With more advanced tumors (invasion into the constrictor muscles), the patient may initially experience odynophagia (painful swallowing) with solid foods or roughage, which may be associated with a a foreign body sensation in the throat. Necrosis or trauma to the tumor bed will produce blood-streaked saliva. Dysphagia (inability to swallow) is produced by bulky tumors that obstruct the food passages or by deep constrictor muscle invasion, prevertebral space invasion, or invasion of the overlying strap muscles. This finding may be associated with salivary drooling, neck stiffness, and a "hot potato" voice. The last finding is due to laryngeal, and especially base of tongue, invasion. Nasopharyngeal and palatal tumor extension produce an air escape speech pattern or nasal voice. Tumor invasion of the larynx, especially with pyriform fossa, aryepiglottic fold, or postcricoid lesions, may result in hoarseness (vocal fold paralysis) and, in rare instances, airway obstruction. A more common cause of hoarseness is direct vocalis or cricoarytenoid joint invasion although it may be associated with recurrent laryngeal nerve invasion. [ref: 39] Approximately 5% to 15% of presenting cases require an emergency tracheotomy (Spector G: unpublished data). Advanced disease causes significant weight loss.
A major neurologic finding is referred pain to the ipsilateral ear, which is referred along the internal branch of the superior laryngeal nerve (sensory division to the larynx and hypopharynx) via the vagus nerve (X) to the auricular branch of the vagus nerve (Arnold's nerve). On rare occasions direct tumor involvement or lymph node extension to the hypoglossal nerve may produce ipsilateral tongue paralysis. On many occasions a cervical mass, usually in the subhyoid region (i.e., jugulodigastric area) (lymph node level II or III), may be the only presenting sign. This is common with small cancers of the pyriform sinus. Postcricoid tumors generally produce pain and obstructive symptoms that are followed by aspiration or vocal cord paralysis. Most patients with hypopharyngeal cancers have poor dentition and halitosis. [ref: 62]
Diagnostic Workup
The initial history and physical examination should include an indirect laryngoscopy and a flexible endoscopic examination under topical anesthesia; in many cases it is coupled with a photographic or video recording of the lesion and all associated areas. Posterior pharyngeal wall lesions may be missed during indirect laryngoscopy.
Small lesions of the pyriform sinus, especially at the apex, may not be noted due to mucosal folds overlapping the lesion, patient gagging, or field movement. Specifically, the inferior extent of most hypopharyngeal tumors is hard to delineate on clinical examination. Some clues to the presence of lesions are pooling of saliva in the pyriform fossa, interarytenoid edema, inability to view the pyriform
fossa due to edema or pooling of secretions, asymmetric constrictions or movements during swallowing, and supraglottic or pharyngeal wall edema.
Radiologic evaluation is very important. Imaging studies should be performed before tumor biopsy and direct panendoscopy to minimize edema. Examination includes a chest x-ray and CT scan with contrast of the head and neck region, which is helpful in delineating cartilage and bone invasion by tumor as well as extralaryngeal and paraglottic tumor invasion. Magnetic resonance imaging (MRI) is more useful in delineating the true extent of the primary tumor and extracapsular lymph node tumor extension. Although contrast laryngography is seldom used today, it was effective in delineating the pyriform apex, subglottic area, vallecula, and esophageal inlet. In most cases in order to delineate the inferior border of the lesion and involvement of the esophageal inlet, a barium swallow including a video for hypopharynx and cervical esophagus evaluation is obtained.
Generally, if no hypopharyngeal tumor is seen in the presence of a neck mass, a fine-needle aspiration biopsy is performed to confirm neck metastases. However, the most important diagnostic evaluation technique is a direct panendoscopy with a biopsy. The entire extent of the tumor, including all margins and potential areas of invasion (as determined by mucosal edema or submucosal elevations), is mapped with both a written and a diagrammatic illustration of the lesion. This description should include the stage of the primary tumor and neck disease as well as documentation of neural deficits and depth of tumor invasion. A systematic approach is required to visualize the entire area including the nasopharynx, oropharynx, oral cavity, and larynx in addition to the hypopharynx. To determine the inferior tumor extent, we generally perform a bronchoscopy and esophagoscopy at the same time.
Staging Systems
The American Joint Committee (AJC) staging system is used most often to stage hypopharyngeal tumors [ref: 5] (Table 41-2). However, there are intrinsic problems when it is applied randomly to the hypopharynx because tumors at different sites have variable behavior and prognoses. For example, we have been able to separate aryepiglottic tumors into two groups; those that deeply penetrate the lateral laryngeal wall and paraglottic space (stage III) have a more favourable prognosis than lesions that spread to the supraglottis or medial pyriform wall (stage II) (Fig. 41-7).
The latter had a 15% decremental prognosis over the entire 20-year follow-up period, irrespective of tumor stage. [ref: 97] Some have suggested a new staging system for aryepiglottic fold tumors. [ref: 92] In general, irrespective of stage, pyriform fossa tumors that involve a single wall have a better prognosis than do those that involve two or three walls in the pyriform apex region (Fig. 41-8). [ref: 99]
We have noted that the AJC system does not separate well survival of pyriform and aryepiglottic fold stage II and III tumors during the first 5 years after treatment; there is a separation at 7 years and thereafter. [ref: 97]
The AJC classification shown in Table 41-2 fails to subdivide the hypopharynx into specific anatomic subsites. Furthermore, the system fails to require tumor size. Both of these variables (tumor site and size) are prognostically significant, particularly in radiation therapy and conservation surgery. At our institution, where over 60% of patients undergo voice-sparing conservation surgical techniques in conjunction with irradiation, we use (internally within the institution) the established Ogura system of hypopharyngeal primary tumor classification, which is particularly helpful in the selection of patients for conservative surgery. [ref: 80]
Pathologic Classification
Over 95% of tumors of the hypopharynx are squamous cell carcinomas. Uncommon varieties of squamous cell carcinomas include basiloid squamous cell carcinoma, superficial spreading carcinoma, sebaceous carcinoma, adenosquamous carcinoma, signet-ring squamous cell carcinoma, and verrucous carcinoma. [ref: 15,28,69,72,88,91] Uncommon nonsquamous cell malignancies include adenocarcinoma, lymphoma, sarcoma (liposarcoma, fibrosarcoma, chondrosarcoma), and malignant fibrous histiocytoma. In a study of 108 patients, we reported that over 60% of the carcinomas were keratinizing, and one third were nonkeratinizing. [ref: 68] Nonkeratinizing tumors were usually poorly differentiated. In a study of 408 pyriform sinus tumors, 23% were well differentiated, 59% were moderately differentiated (i.e., 82% had some keratinization), and 18% were poorly differentiated. [ref: 99] In 315 patients with aryepiglottic fold tumor involvement, there were 47% well differentiated, 41% moderately differentiated, and 12% poorly differentiated tumors. [ref: 97] These differentiations had no prognostic significance. [ref: 97,99]
The tumor margins are generally infiltrating in 80% and pushing in 20% of specimens studied. [ref: 68] We noted that, in aryepiglottic fold tumors, localized pushing lesions had a 15% better prognosis than did diffusely infiltrative lesions. [ref: 97] However, in general, the degree of keratinization and differentiation, the type of tumor margins, and the pattern of perineoplastic stromal activity had no
significance in terms of prognosis or nodal metastases. [ref: 68,97,99]
Over 95% of malignant tumors of the hypopharynx are epithelial in origin (i.e., squamous cell carcinomas of various degrees of differentiation). Typically, these carcinomas have extensive involvement of the epithelium with ulceration (Fig. 41-9).
Skip lesions or multifocal presentations are not unusual. The tumor borders are highly infiltrative and induce a desmoplastic reaction. Most
hypopharyngeal tumors present as wide shallow ulcers with a variable degree of deep invasion and extensive submucosal spread (Fig. 41-10).
Whole-organ sections of the pyriform fossa have demonstrated unsuspected submucosal tumor spread well beyond 1 cm of the visible tumor margins. [ref: 57,58] Most tumors do not have significant keratosis or epithelial maturation; thus, the incidence of well-differentiated tumors in the hypopharynx is less than 40%. [ref: 97,99]
Squamous cell carcinomas with a pseudosarcomatous reaction (i.e., spindle cell carcinomas) have a slightly better prognosis than poorly differentiated tumors. Tumor recurrence in the pharynx and neck is more common with keratinizing than nonkeratinizing tumors, tumors with invasive margins rather than pushing margins, soft tissue extension, extracapsular lymph node extensions, and positive surgical margins. [ref: 63] Distant metastases are more common with poorly differentiated, nonkeratinizing carcinomas, lymph node metastases, and uncontrolled primary site disease. [ref: 63] Pathologic findings that adversely affect survival are positive surgical margins or tumor persistence in the irradiation field following initial definitive therapy in pyriform fossa tumors (Marks J: unpublished data, 1978). The margins of resection are more often negative with preoperative irradiation (7.7%) than with resection followed by postoperative irradiation (16.7%) (Marks J: unpublished data, 1978).
Prognostic Factors
Age and gender are two host factors that have prognostic significance in hypopharyngeal (specifically aryepiglottic fold and pyriform fossa) tumors. Survival progressively declines with increasing age, and women have a significantly higher survival rate 3 to 20 years after therapy, [ref: 97,99] primarily because of lower T stage (70% are T3 or less) and N stage neck metastases (79% are N0 or N1) at presentation. [ref: 97,99] For example, most women (more than 70%) with pyriform sinus cancer had T1-3 and N0-1 disease. [ref: 97,99] There is a more favorable result in the younger population (Ellis W, Marks J: unpublished data, 1978). [ref: 24,27] However, the incidence of hypopharyngeal cancers in patients who are under 40 years of age is small (1% to 3%); the latter present with stage IV disease in over 50% of cases. [ref: 30,102] There is a borderline significance for favorable survival in the younger population, primarily because of lower T stage and N stage at presentation. However, younger patients have a higher risk for secondary malignancies. [ref: 90]
Race is also important. Generally, young patients, women, and white Americans have higher cure rates. African-Americans have a 26% lower survival than do whites after treatment of pharyngeal cancers; the incidence of hypopharynx cancer is higher in this group. [ref: 5]
Generally, patients with weight loss, malnutrition, cachexia, anemia, pulmonary disabilities (emphysema), and liver dysfunctions (cirrhosis) do poorly. Anatomic location of the primary tumor, tumor size, and presence of metastases in the neck best correlate with prognosis. [ref: 97,99]
Aryepiglottic fold and medial wall pyriform fossa tumors are usually smaller and more localized, which leads to higher cure rates than with postcricoid and pharyngeal wall tumors. [ref: 97,99] Small tumors (T1N0 and selected T2N0) at any hypopharyngeal site have higher cure rates and local control and better prognosis than do larger lesions (even if treated by unimodality therapy). [ref: 97,99] In the pyriform sinus, one-wall tumors have a higher cure rate than medial wall and aryepiglottic fold tumors. [ref: 97,99] The poorest results are seen with pyriform apex, postcricoid, and two- or three-wall tumors. There is a significant decrease in cure rate with T4 and N3 disease at all hypopharyngeal sites. [ref: 97,99] The presence of neck metastases reduces the survival rate by 28%. [ref: 97,99] Metastatic capsular rupture of the nodes (extracapsular spread to soft tissues) or N2 or N3 disease decreases survival by an additional 12%. [ref: 97,99]
The degree of tumor differentiation does not have prognostic significance; however, certain trends are apparent in that keratinizing tumors with infiltrating margins are associated most often with locoregional failure, and nonkeratinizing lesions that are poorly differentiated have a higher distant metastatic rate.
Other poor prognostic signs are positive surgical resection margins or tumor persistence in the irradiated volume. These are usually unsalvageable candidates, although radical surgery for radiation persistence in pyriform sinus tumors is effective in 44% of cases, and radical irradiation for surgical persistence is 32% effective. [ref: 25] These are not statistically significant differences because these salvages represent different initial tumor stages. [ref: 97,99]
A variety of tumor biologic factors have been studied to determine prognosis. Recent studies demonstrated that hypopharyngeal tumors with detectable human papillomavirus (HPV) DNA had a decremental survival that is independent of tumor stage. Only a small subset of hypopharyngeal cancers have HPV DNA, and this may represent a small biologic subset of tumors carrying a poorer prognosis. [ref: 19,104] Squamous cell carcinoma of the hypopharynx that expressed the p53 suppressor gene was found in younger patients, was associated with advanced tumor stage disease, and had increased expression of epithelial growth factor receptors. There was no correlation with multiple primary tumors, tumor grade, DNA ploidy, or percentage of S phase. [ref: 17,33] The role of tumor cell ploidy, which is considered to be a predictor of survival in some tumors, is controversial in head and neck malignancies. [ref: 1,100] In addition, the expression of epithelial growth factor receptors was not predictive of survival. [ref: 32] In general, hypopharyngeal tumors are nondiploid, as are two thirds of all head and neck malignancies. Tumors that are poorly differentiated tend to be nondiploid. [ref: 100] Some have tried to determine prognosis or tumor invasiveness by evaluating the serum and urine of patients with hypopharyngeal tumors; sedimentation rate, thymidine kinase, hydroxyproline, lipid-bound sialic acid, prostaglandin E, histamine, and other by-products were of marginal or no value. [ref: 31,49] Others have studied the expression of the nuclear organizer region, histocompatibility antigens, laminin, and laminin-associated glycoprotein synthesis and secretion without success. [ref: 29,36,42,52,98] Most agree that today there is no specific prognostic marker, [ref: 38,107] and none is quantitative for tumor burden or biologic tumor behaviour Molecular prognostic markers in squamous cell carcinoma of the head and neck: the role of E-cadherin..
General Management
The best treatment for hypopharyngeal carcinomas is that which achieves the highest local and regional control rate with the least functional damage. The functions that need to be preserved are respiration, deglutition, and phonation, if possible, with the least risk to the host and without the use of permanent prosthetic devices. In general, most T1N0 and selected T2N0 lesions can be treated equally well with curative irradiation or conservation surgery. [ref: 26,97,99] Invasion of the larynx by a pyriform fossa tumor with vocal cord fixation predicts a poor outcome to curative irradiation. [ref: 4,96] Larger lesions and neck metastases require combined surgical resection and adjuvant radiation therapy. Data suggest that preoperative or postoperative irradiation provides equally good tumor control. [ref: 97,99] However, postoperative adjuvant irradiation is associated with less morbidity and fewer complications of therapy and therapy-related deaths. [ref: 97,99] Because most of our patients have advanced primary (more than 60% T3 and T4) and regional nodal (more than 68% N+) disease and because most lesions are understaged at presentation, our approach has been to use combined surgery and postoperative irradiation for almost all lesions. [ref: 26,97,99] Table 41-3 outlines the management of hypopharyngeal tumors.
The efficacy of chemotherapy, used in a triple-therapy mode for organ preservation and aiming at improved survival, remains unproven. [ref: 56,93] Chemotherapy may have a significant potential for future treatment of hypopharyngeal cancers because of the high incidence of locoregional failure (25% to 30%) and distant metastases (more than 18%). [ref: 26,97,99] In a study of advanced disease using platinum-based induction chemotherapy and irradiation, a response rate of 78% was achieved, with 28% of patients preserving the larynx and 46% surviving tumor free at least 2 years. [ref: 93] Keane and associates [ref: 51] showed no advantage in local control or survival for split-course irradiation and concurrent chemotherapy with mitomycin-C and 5-fluorouracil compared with radiation therapy alone. In another study of cisplatin and bleomycin in both concomitant and neoadjuvant roles in stage IV head and neck cancers compared with radical radiation therapy alone, chemotherapy produced a higher tumor response rate but also a greater complication rate. Ultimately, there was no improvement in overall survival rates (P = 0.706). [ref: 87] Immunotherapy and cell-mediated immunity have been ineffective. [ref: 13]
Surgery When surgery is contemplated, every attempt is made to preserve the patient's functions. In conservation surgery a more precise delineation of the lesion with biopsy mapping of the primary tumor is of paramount importance. Conservation surgical procedures take into account the size and location of the lesion as it is related to the specific organ function at risk, the fixation or mobility of the cervical lymph nodes, and the medical condition of the patient. Contraindications for conservation surgery include the following: transglottic extension, cartilage invasion, vocal fold paralysis, pyriform apex invasion, postcricoid invasion, and extension beyond the laryngeal framework. [ref: 97,99] In all cases, at a minimum, an ipsilateral neck dissection is performed (functional, modified, or
radical resection), almost always followed by postoperative radiation therapy. Advanced posterior hypopharyngeal wall tumors generally are treated with bilateral modified radical neck dissections. To resect the primary pharyngeal tumor, the larynx is rotated anteriorly, preserving the neurovascular supply. The pharyngeal wall is resected to include the prevertebral fascia under frozen-section control. The area is reconstructed, usually with a free radial forearm flap, opened jejunal free flap, or less frequently with a myocutaneous flap. Tumors of the aryepiglottic fold are resected with an extended subtotal supraglottic laryngectomy and neck dissection if they fulfill the resection criteria of not extending beyond the larynx, transglottic extension, or vocal cord paralysis. Extension into the base of the tongue, epiglottis, and vallecula can be handled by extension of the operative field superiorly to resect these lesions and portions of the base of the tongue. In such cases we reconstruct the defect with myocutaneous flaps. Generally, the superior laryngeal nerves are sacrificed, which may lead to silent aspiration. A team of speech therapists facilitates swallowing education, and nutritionists define
the texture and caloric content of the diet.
Small bulky lesions confined to the medial and anterior pyriform fossa walls or aryepiglottic folds that do not extend to the pyriform apex, beyond the larynx, postcricoid, vocal cord (paralysis), and contralateral arytenoid and occur in patients who do not have pulmonary and cardiac disabilities are amenable to partial laryngopharyngectomy and neck dissection. This approach is not possible if the tumor extends to the pyriform apex, which may lie below the level of the vocal cords or the lateral pyriform fossa wall, which usually traverses the thyroid ala and has extralaryngeal spread. [ref: 39,54,68,97,99] The use of vascularized tissue for reconstruction has reduced our overall complication rate from more than 30% to 18% and the therapy-related mortality rate from more than 7% to 2.4%. [ref: 97,99] Over two thirds of our patients receiving combined therapy for pyriform fossa tumors (207 of 302 patients [69%]) underwent conservation surgical procedures with preservation of vocal function, swallowing, and normal respiration. [ref: 97] A small group of patients require tracheotomy or completion laryngectomy for chronic aspiration or prolonged gastric tube feeding (less than 3%). However, over 60% of patients had minimal silent aspiration. Conservation procedures are not advocated in elderly, pulmonary compromised, and neurologically deficient patients. In patients who do not meet the criteria for conservation surgery, either a total laryngopharyngectomy or a total laryngectomy and partial pharyngectomy with reconstruction in conjunction with neck dissection are performed. In general, patients with tumors of the postcricoid area who do not respond to curative irradiation need to have a total laryngopharyngectomy and neck dissections. On rare occasions, the anterior laryngeal framework can be preserved to allow for a laryngotracheal autograft repair. [ref: 39,40] If the dissection of any hypopharyngeal tumor includes the entire hypopharynx and the esophageal inlet, then a gastric pull-up procedure is used for neopharyngeal reconstruction. [ref: 40] In the past, colon transpositions were popular techniques. [ref: 6] However, unless there is a second primary tumor in the thoracic esophagus or stomach, the technique is no longer favored. [ref: 40]
Irradiation Alone Irradiation alone controls a substantial proportion of small surface lesions in the pyriform sinus. [ref: 4,75,78] Mendenhall and associates [ref: 75] reported that 16 of 25 T1 and T2 lesions of the pyriform sinus (64%) were controlled with irradiation alone (65 to 70 Gy in 7 to 8 weeks). If irradiation alone is to be used, it is important that the radiation oncologist be present at direct pharyngoscpy or review the video laryngopharyngoscopy findings. The best results are obtained by selecting lesions that are confined to one or two walls of the pyriform sinus, lack bulk, and do not infiltrate the larynx or destroy thyroid cartilage.
Surgery and Irradiation Patients with advanced bulky tumors that fill the pyriform sinus, invade the larynx, destroy thyroid cartilage, and extend into the soft tissues of the neck require total laryngopharyngectomy, radical neck dissection, and adjuvant irradiation.
Higher doses of adjuvant irradiation (60 to 66 Gy) are better delivered postoperatively than preoperatively because preoperative irradiation (usually 45 to 50 Gy in 4.5 to 5 weeks) may retard healing of pharyngeal and cutaneous suture lines and may cause more complications than postoperative irradiation. [ref: 12,22,106] Preoperative irradiation is advised for patients with fixed lymph nodes because neck dissection is later possible in some of these patients. [ref: 65] Preoperative irradiation need not increase postsurgical complications, provided sufficient time is allowed between radiation therapy and surgery for fibroblasts to repopulate
the irradiated field. [ref: 63]
In pyriform fossa tumors, combined therapy had higher cure rates (71%) than did surgery (53%) or irradiation (27%). [ref: 97] There was no statistical difference in the sequencing of irradiation and surgery; preoperative and postoperative irradiation produced equal results [ref: 99] (Table 41-4). The same was true with aryepiglottic fold tumors, in which combined therapy (68%) had better disease-free results than surgery (61%) or radiation therapy (34%) at 5 years [ref: 97,99]; surgical cases were more favorable smaller lesions, and the radiation therapy cases had more advanced diseases. The use of combined therapy with irradiation given in the adjuvant postoperative mode and surgical reconstruction performed with fresh nonirradiated tissue brought into the treated field with pedicled flaps (rare), myocutaneous flaps (most common), or free flaps (most common today) reduced the complication rate from more than 20% to 5% and the therapy-associated death rate from more than 7% to 2.4%. [ref: 16,34,97,99]
Pharyngeal Wall Cancers During the early 1970s, our policy of treatment of pharyngeal wall cancers was low-dose preoperative radiation therapy (30 to 40 Gy in 3 to 4 weeks), followed by surgery. In patients who were not surgical candidates, radiation therapy alone was the treatment of choice. [ref: 64,66] An analysis by Marks and co-workers [ref: 64] showed 43% locoregional tumor control and over 50% major postsurgical complications with a 14% mortality rate with preoperative low-dose irradiation followed by surgery. Meanwhile, others reported better tumor control and fewer complications with irradiation alone. [ref: 77,110] Therefore, low- dose preoperative irradiation followed by surgery was discontinued in our institution in 1978, and patients with pharyngeal cancer were treated with irradiation alone. Analysis of patients treated with irradiation alone between 1978 and 1982 showed a very poor rate of primary tumor control (25%), [ref: 66] even with doses of 65 and 70 Gy. Since then, the policy has been wide resection of the primary tumor, ipsilateral modified neck dissection, and closing of the pharynx with a myocutaneous flap, followed by high-dose postoperative radiation therapy after healing of the pharyngeal and cutaneous suture lines. The dose is 60 Gy in 6 weeks with an additional 6 Gy for close margins or extracapsular extension of the given nodal site. A recent analysis by Emami and colleagues [ref: 26] showed that combined therapy had a significantly superior cure rate of 49% to low-dose preoperative irradiation and surgery (22%) or definitive radiation therapy (7%) at 5 years.
External-beam irradiation of pharyngeal wall cancer yields rates of tumor control of 21% to 50%. [ref: 66,75,77,83,110] Tumor control is better for small than for large tumors and is enhanced by interstitial implantation with **192Ir or **125I. [ref: 75,95] Son and Kacinski [ref: 95] controlled 12 of 14 pharyngeal wall cancers for 6 to 88 months after external irradiation and implant with **192Ir or **125I. They described the implantation technique and reported necrosis of the primary tumor and reepithelialization of the pharyngeal wall. Ulceration and fibrosis of the pharynx were not mentioned.
Postcricoid Cancers Most postcricoid cancers managed by radiation therapy show dismal results. [ref: 30,48,59,60,112] In a series of 200 patients, 25% were not treated, 25% were irradiated with palliative intent, and the remaining 50% received irradiation with curative intent [ref: 30]; all untreated patients were dead within 9 months, and only 20% of those definitively irradiated survived 5 years. There is decreased survival with increasing tumor length and fixation of the vocal cord. [ref: 30,112] Stell and associates [ref: 101] observed that survival was extremely poor for lesions that were greater than 5 cm in vertical length, which were associated with bilateral nodes, nodal fixation in the thoracic inlet, and invasion of the esophageal inlet. Pearson [ref: 82] noted, in a controversial study of a group of carefully selected patients, a 30% 3-year survival rate with radical irradiation. A more realistic rate of 13% 3-year survival has been reported by others. [ref: 45] Harrison, [ref: 40] reporting on more than 200 patients treated with combined therapy, found that a gastric pull-up procedure after total laryngopharyngectomy and neck dissection and radiation therapy yielded the most successful results.
Recurrent Tumors Treatment of tumor recurrences of the hypopharynx is equivalent for radiation therapy and surgery. [ref: 25,97,99] Generally, salvage is higher after single-modality definitive therapy (less than 60%) than combined definitive therapy (31% to 44%) in pyriform fossa and aryepiglottic fold tumors. [ref: 97,99] The salvage rates for irradiation or surgery failures are approximately equal. The success in salvage therapy is usually greater with completion laryngopharyngectomy and contralateral neck dissection for delayed metastases. [ref: 105] Salvage for positive resection margins or persistent disease in the postirradiation setting is notoriously poor. Neck recurrences after combined therapy have an especially poor outcome. [ref: 25] Most patients die within 1 year of treatment.
The risk of secondary malignancy developing after primary tumor control varies with different studies and may be as high as 26%. [ref:48] In our series of patients with pyriform fossa and aryepiglottic fold tumors, the incidence of secondary malignancies was 6% to 8%; the most common sites were lung and oropharynx. [ref: 97,99]
Radiation Therapy Techniques
Preoperative Irradiation Radiation therapy is delivered to the larynx, pharynx, and neck. Lateral fields extend from the base of the skull and mastoid to the supraclavicular lymph nodes and encompass the anterior and posterior cervical lymph node chains. For pyriform sinus cancer that extends superiorly into the oropharynx, fields are designed to encompass retropharyngeal nodes up to the base of the skull. Preoperative doses are 45 to 50 Gy given in 4.5 to 5 weeks.
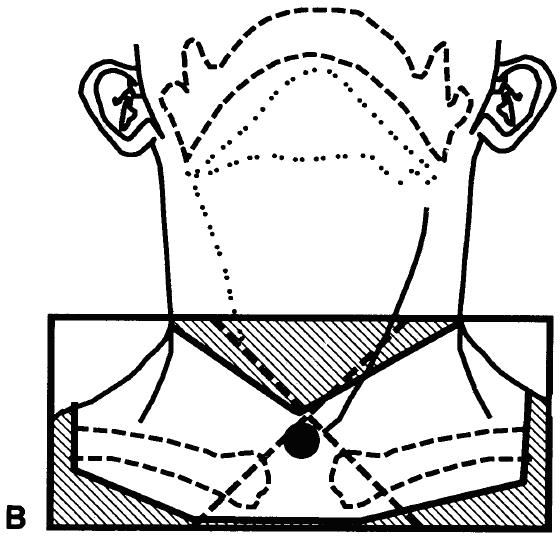
Postoperative Irradiation Postoperative irradiation for hypopharyngeal tumors is designed to prevent recurrence in the laryngeal remnant, pharynx, tracheostoma, and cervical lymphatics. A dose of 60 Gy is routinely prescribed after successful extirpation of the tumor. If the pathologist demonstrates tumor in the margins of excision or if there is extracapsular extension of a node in a given cervical nodal region, an additional 6 Gy is delivered to the high-risk area. The technique most commonly used consists of three fields: opposed upper lateral fields, encompassing the primary tumor from the base of the skull, and upper cervical lymph node and anterior low neck field to irradiate the tracheostoma and lower cervical lymph nodes (Fig. 41-11).
The spinal cord is shielded at the junction of the upper and lower fields from the lateral portals just posterior to the pharynx (Fig. 41-12).
An anterior shield is not used, to avoid shielding of the pharynx, tracheal lymph nodes, and parastomal tissues. At our institution, an asymmetric jaw technique for the arrangement of both lateral upper necks and/or a beam-splitter for the low neck field is routinely used to prevent upward divergence of the radiation beam and possible overlap at the junction of the three irradiation fields. A small notch on the posterior and lower corner of the lateral fields ensures no overlap over the spinal cord (Fig. 41-12).
Compensating filters are required for low-energy megavoltage beams to eliminate dose inhomogeneity that results from variations in thethickness of the neck. The entire spinal cord is shielded after 42 to 44 Gy, and the posterior neck underlying the shield is irradiated with a 9-MeV electron beam to complete the dose to the desired level (Fig. 41-13).
In patients with pharyngeal wall primary tumors, if the anterior cervical nodes are negative radiographically or pathologically, posterior triangles need not electively be irradiated. Therefore, the posterior border of the field can be placed at the posterior edge of the vertebral bodies (Fig. 41-13).
Irradiation Alone Only very selected patients with very early tumors of the hypopharynx are treated with irradiation alone. The irradiated volume should encompass nasopharynx, oropharynx, hypopharynx, and upper cervical esophagus because of the propensity of these cancers to spread submucosally. [ref: 39] The technique, consisting of two parallel opposed upper neck lateral beams and one anterior field encompassing the low neck, is similar to that described for postoperative irradiation. The patient usually pulls on a strap looped around the feet to depress the shoulders. The location of the anterior border for the upper neck portals may vary according to the tumor extent and location; in most cases, the anterior border does not flash the skin of the neck. The anterior third of the glottis can usually be shielded in patients with posterior pharyngeal wall tumors. The boost volume (after 60 Gy) should encompass the gross tumor (and grossly involved nodes) up to an additional 10 to 15 Gy. The total prescribed dose is about 70 to 75 Gy in 8 weeks. If an altered fractionation regimen is used, the total dose will be higher (see Results of Therapy).
Dose Response Pyriform Sinus Cancers Improved primary tumor and nodal control with increasing doses has been documented for primary T1 and T2 cancers of the pyriform sinus and involved lymph nodes, regardless of size (Fig. 41-14).
The dose-response curve for small tumors plateaus after 70 Gy and is flat for larger T3 tumors within the therapeutic range of doses used. There seems to be a moderate advantage to increasing the dose for small tumors and lymph nodes, but there is no advantage in delivering doses up to 70 Gy for T3 cancers of the pyriform sinus because higher doses are necessary to improve tumor control.
Pharyngeal Wall Cancers Improved tumor control with increasing doses of irradiation has been reported for T1 and T2 pharyngeal wall cancers, but the dose-response curve for advanced T3 and T4 lesions is relatively flat within the range of doses reported (Fig. 41-15).
Exophytic pharyngeal wall cancers are probably more radioresponsive and easier to control than endophytic ulcerating tumors. Doses of 65 to 75 Gy administered in 6.5 to 7.5 weeks are recommended for T1 and T2 lesions to achieve maximal tumor control without excessive complications. [ref: 67] Doses in excess of 70 Gy delivered in 6.5 to 7 weeks are not advantageous for advanced ulcerated tumors because control of more advanced tumors is unlikely and radiation-induced complications are more common. [ref: 67]
Results of Therapy
The overall cure rate for hypopharyngeal tumors is 55% with the following distribution of cure rates: 80% local disease, 43% regional disease, and 20% distant disease. [ref: 2,5] The cure rates among African-Americans are lower, with an overall cure rate of 34% and specific cure rates as follows: 69% local disease, 30% regional disease, and 12% distant disease. Nevertheless, there has been an overall statistically significant improvement (P < 0.05) in cure rates in the years between 1974 and 1976 and 1983 and 1990. The 5-year overall cure rates increased from 45% to 56%. [ref: 4,8] Because these data include survival statistics for the entire pharynx, specific data for the hypopharynx (incidence and mortality) are less well reported. Our data indicate that the cumulative disease-free 5-year survival rates were similar to those projected for the entire pharynx; the 5-year disease-free survivals were 66% for aryepiglottic fold tumors, 55% for pyriform sinus tumors, and 49% for hypopharyngeal wall lesions. [ref: 16,97,99]
Most of our patients presented with advanced-stage disease. In this group of patients, the results of combined surgery and radiation therapy are superior to those with irradiation alone for cancers of the pyriform sinus and pharyngeal wall. [ref: 26,99] In patients with pyriform sinus tumors, there was no difference between the results of preoperative irradiation and surgery versus surgery followed by postoperative radiation therapy (Table 41-4), whereas in patients with pharyngeal wall cancers, results with postoperative irradiation were significantly superior to those with low-dose preoperative irradiation followed by surgery. [ref: 26] In pyriform sinus tumors, the 5-year disease-free survival was affected by the extent of the tumor; in patients with one involved wall, the 5-year survival rate was 73
compared with 49% when two or three walls plus the apex were involved (Table 41-5). Similarly, patients with lateral pharyngeal wall tumors did better than those with posterior pharyngeal wall lesions, and both groups did better than patients with involvement of the posterolateral wall.
Treatment results are summarized in Table 41-6 and Table 41-7. The ability to control the primary tumor and lymph nodes progressively diminishes for carcinomas of the pyriform sinus, pharyngeal wall, and postcricoid region, an observation explained by tumor respectability and size (Fig. 41-16) (Ellis W, Marks J: unpublished data, 1978). [ref: 64,65]
Pyriform sinus cancer, because of its anterior and superior location in the hypopharynx, is more easily resected and controlled than are the posteriorly and inferiorly located cancers of the pharyngeal wall and postcricoid region. Control of pharyngeal wall cancers by radiation therapy progressively declines with advancing T stage or tumor size; postcricoid or epiesophageal tumors are often larger and more difficult to control than pharyngeal wall cancers. [ref: 60,77]Value of PET scan in treatment decision making for nodal metastases in SCHNC-single institutional update.
Sequelae of Treatment
Because of the aggressive nature of hypopharyngeal tumors, radiation therapy and surgery frequently are used together, and complications have been significant (Table 41-8 and Table 41-9). [ref: 37] It is apparent from both retrospective and prospective studies that the incidence of major complications, including carotid rupture, is usually greater for preoperative than for postoperative irradiation. [ref: 12,21,106] The incidence of pharygocutaneous fistulas after pharyngectomy is the same whether the pharynx has been irradiated before or not, but the time required to heal a preoperatively irradiated fistula is significantly greater than for an unirradiated fistula. [ref: 12,106] Although there was no statistical difference between preoperative or postoperative irradiation, postoperative irradiation with flap reconstruction decreased the incidence of all complications, especially perioperative or delayed fatal complications (from 20% to 5.7%).
Balancing risk with benefit is essential in determining the optimal treatment strategy for any hypopharyngeal tumor. Surgery-related mortality after low-dose preoperative irradiation and pharyngectomy for cancers of the pyriform sinus and pharyngeal wall ranges from 10% to 14%. [ref: 35,64] A mortality of this magnitude is acceptable for cancer of the pyriform sinus because the probability of primary and nodal control exceeds mortality by a factor of six, and survival exceeds mortality by a factor of three. [ref: 65] For pharyngeal wall cancers, however, a mortality of this magnitude is unacceptable because it is roughly equivalent to survival, and irradiation alone gives the same rate of primary and nodal control as surgery without the associated mortality. [ref: 64]
Clinical Trials Clinical research for hypopharyngeal cancer can arbitrarily be divided into three categories: altered fractionation, combined chemoirradiation, and improved delivery of irradiation therapy (three-dimensional conformal irradiation). Although numerous institutional reports of phase II trials indicate improved results with hyperfractionation [ref: 44,75] or accelerated hyperfractionation [ref: 84,109] in patients with head and neck cancers, in which a subset of patients harbor hyperpharyngeal tumors, no randomized study has shown superiority of altered fractionation over conventional fractionation in terms of local tumor control or survival in patients with tumors of the hypopharynx. Currently, a Radiation Therapy Oncology Group (RTOG) study is attempting to answer this question; standard fractionation is being tested in a randomized fashion against various forms of altered fractionation in patients with inoperable head and neck tumors.
The results from institutional phase II trials using combination chemoirradiation are even more controversial in patients with head and neck cancer. Although aggressive chemoirradiation regimens have resulted in improved control rates and survival (Abitol et al, personal communication), they also have resulted in significantly increased acute and long-term complications. Several randomized
studies have failed to show any improvement when chemotherapy is added to standard radiation therapy. Currently, a phase III trial is being conducted by the RTOG in which patients with operable head and neck cancers (hypopharynx included) with high-risk prognostic factors are randomized to be treated with standard postoperative radiation therapy or postoperative chemoirradiation (platinum-based combination chemotherapy). The research on improved planning and delivery of radiation therapy via three-dimensional conformal irradiation technology is at the early stages of research and is mainly aimed at decreasing short- and long-term complications. These studies undoubtedly will have a significant impact on the future management of patients with hypopharyngeal cancer.